[This “sponsored content” article was published on bostonglobe.com on February 2nd.]
Six years after the Affordable Care Act (ACA) became law, U.S. health care policy and the delivery of medical services continue to undergo unprecedented change. Rockland Trust’s “Talking Business Advice Series” spoke with John E. McDonough, professor of Public Health Policy at the Harvard T.H. Chan School of Public Health, to get his take on what may lie ahead for businesses working with the ACA during this dynamic period.

Q: You helped write the ACA. It’s an extremely complex law that even today is not fully understood by many Americans, including business owners and leaders. From a high-level perspective, where do things stand with it today?
A: Most people understand that the ACA is moving us toward universal health coverage. For the United States, the ACA is a revolution, an enormous set of changes that many see as a huge step forward and many others see as a wrong turn. Globally, however, all of the world’s advanced nations prior to the ACA already had health care schemes that, to varying degrees, met the insurance needs of their populations. So, while the ACA’s insurance expansions and reforms represent a great leap forward for the U.S., it is also true that when fully implemented by 2018, the U.S. will still have the most inefficient, wasteful, and unfair health insurance system of any advanced nation, even with the ACA reforms.
On the other hand, the ACA is also advancing an agenda of dramatic and necessary change in how medical care is delivered in the U.S. As a nation, we are now moving rapidly away from a financing system based on fee-for-service payments, (which is) a system that rewards hospitals, physicians, and other medical providers based on the quantity of services they provide without regard for the quality, effectiveness, and efficiency of those services. Because of the ACA, we are now moving quickly toward a new financing framework that rewards hospital, physicians, and providers based on the quality and value of the services they provide rather than the quantity.
Q: The public doesn’t necessarily view it in this way, does it?
A: You’re right. This change has gone unrecognized by the broad public, even as it moves forward in rapid and profound ways. A lot of what the ACA envisions is experimental. Some elements are working better than others; some continue to be fiercely debated. The U.S. doesn’t have all the answers in this effort, but we have the most dynamic set of experiments on this evolutionary path of any advanced nation on the planet right now. Health system leaders all around the world are very interested in this set of experiments and watching closely. That is something that corporate leaders, regardless of industry sector, ought to recognize, appreciate, and understand.
Q: What are some of the effects of these experiments on businesses?
 A: The immediate effects of the ACA depend on the context of the business itself. For example, the ACA’s impact is different for larger businesses with more than 50 full-time workers, companies with new responsibilities under the ACA’s employer mandate. It’s different for smaller employers and it provides some opportunities for many of them. It’s a unique new context for start-up businesses because of the health insurance marketplaces that provide new businesses with a new way to provide health insurance for their workers, enabling them to outsource their health coverage needs for themselves and their employees. And it enables all employees to get health care coverage regardless of pre-existing conditions, which was not possible in 45 states prior to the ACA.
A: The immediate effects of the ACA depend on the context of the business itself. For example, the ACA’s impact is different for larger businesses with more than 50 full-time workers, companies with new responsibilities under the ACA’s employer mandate. It’s different for smaller employers and it provides some opportunities for many of them. It’s a unique new context for start-up businesses because of the health insurance marketplaces that provide new businesses with a new way to provide health insurance for their workers, enabling them to outsource their health coverage needs for themselves and their employees. And it enables all employees to get health care coverage regardless of pre-existing conditions, which was not possible in 45 states prior to the ACA.
So it’s contextual. It depends on the size and nature of the business as to whether there will be advantages or disadvantages—or both—to the Affordable Care Act.
Q: Would you expand on how smaller companies can outsource their health care responsibilities?
A: The ACA required the development of government-regulated health care exchanges (or marketplaces) across the nation. States had right of first refusal and 13 have chosen to establish their own exchanges while the rest are run by the U.S. Centers for Medicare and Medicaid Services (CMS). These exchanges offer coverage to all eligible individuals who can’t obtain insurance elsewhere, and many workers are eligible for financial subsidies to keep premiums and cost sharing affordable.
Alongside these public exchanges, new private health insurance exchanges have emerged. Unlike the public exchanges, which largely provide insurance to individuals seeking to buy non-group coverage, these private entities are aimed straight at the employer community. These private exchanges can enable employers to address their responsibilities under the ACA’s mandate to provide health insurance for their workers and do it in ways that are far less onerous for employers than in the past. It’s a way to outsource these responsibilities and to provide employees with a range of coverage choices. This is a significant change from the environment that existed prior to the ACA’s passage in 2010.
Q: How are larger businesses affected by the ACA?
A: Prior to the ACA’s passage, larger businesses were concerned about not being heavily shaped by the new law because most of these businesses already covered most of their employees. The impact of the ACA on larger businesses—especially those that self-insure—is far less than what they would experience in the standard commercial insurance market were they to go out and purchase traditional coverage.
Nonetheless, there are important new coverage requirements that impact the large employer market—whether self-insured or not. For example, lifetime or annual benefit limits on workers coverage is no longer permitted. Employer plans must cover the “essential health benefits” specified in the law. A worker’s insurance premium cannot exceed 9.5 percent of his or her household income or else the employer mandate penalty can be triggered. All employers must allow their workers to keep adult children on their family policies up to age 26. The ACA also sets a 90-day maximum waiting period before full-time workers are eligible for coverage.
There are also some elements of the law that many employers appreciate, including the ability to vary worker premiums by 30-50 percent in relation to workers’ use of tobacco products and participation in workplace wellness programs. Clinically proven preventive care services, such as mammography, must be provided to workers without any cost sharing.
The ACA’s impact is far more substantial in the traditional commercial health insurance market—but the impact on large self-insured employers is also meaningful.
Q: Are all the details of the ACA settled at this point?
A: This law is changing every day. There are at least three dozen things changing in relation to this law almost daily—in Congress, in federal agencies, in states, in the private sector—changes shaping how this law is unfolding across American society. And the pace of change hasn’t slowed, even now when we’re in the sixth year since the law was enacted.
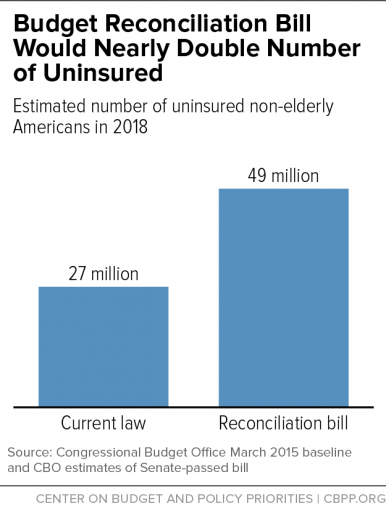
 The ACA is likely to change even further next January when a new president and administration takes office, regardless of which party controls the White House and Congress. We can see an evolving agenda for changes from both sides of the political spectrum. Congressional Republicans have been united in their determination to dismantle the ACA for some time. In January, President Obama vetoed an attempt to cripple the ACA that was included in a budget reconciliation bill. The fact that this initiative passed Congress demonstrates that if Republicans control the White House, House, and Senate next January, there is a strong likelihood of significant dismantling of the law.
The ACA is likely to change even further next January when a new president and administration takes office, regardless of which party controls the White House and Congress. We can see an evolving agenda for changes from both sides of the political spectrum. Congressional Republicans have been united in their determination to dismantle the ACA for some time. In January, President Obama vetoed an attempt to cripple the ACA that was included in a budget reconciliation bill. The fact that this initiative passed Congress demonstrates that if Republicans control the White House, House, and Senate next January, there is a strong likelihood of significant dismantling of the law.
Conversely, if the Democrats hold the White House next year they also will have an agenda for significant changes to the ACA, though far less dramatic than what would happen under Republican control. Either way, we can anticipate some significant changes coming in 2017.
Q: How do business leaders prepare for that?
A: They need to keep abreast of whatever changes occur. Many organizations help businesses to stay on top of what’s changing or likely to change. It’s important for executives and managers who focus on a company’s health coverage to stay up-to-speed on what’s happening, and it’s important for those in the C-suite to understand the changes to factor these new variables into their strategic planning calculus.
As a nation, we are on a path of rapid and deep systemic change to our health system, and it’s going to unfold for some time to come. It is already transforming the fundamental nature of the U.S. medical care delivery system. The implications of it are vast and it will continue to unfold well into the future in positive, not-so-positive, and surprising ways.
It’s important for corporate executives to understand the nature of these changes as they happen.
The Harvard T.H. Chan School of Public Health will present a conference titled “Beyond the Affordable Care Act: The Next Frontiers for US Health Reform” on April 25-27. Visit https://ecpe.sph.harvard.edu/ for more information.