[The Q&A below was published in Harvard media this past week.]
How might the election of Donald Trump as the next U.S. president impact public health over the next four years? John McDonough, professor of the practice of public health at Harvard Chan School, who worked in the Senate on the passage of the Affordable Care Act (ACA), offers his perspective in this Q&A.

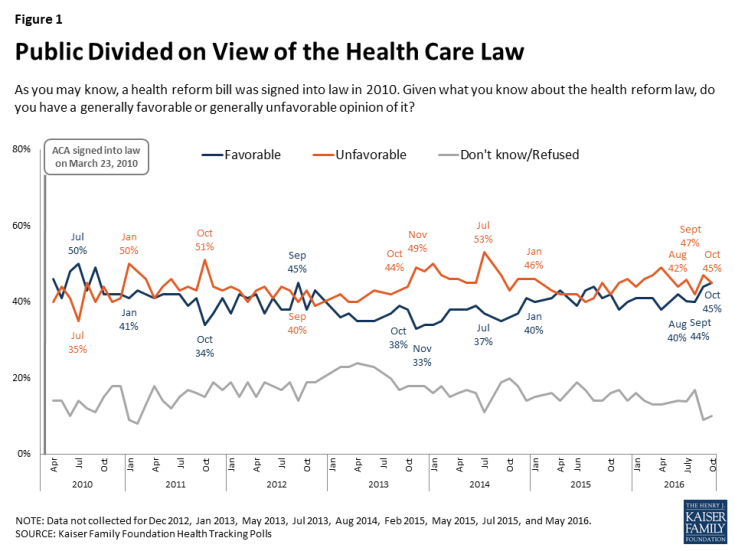
Many are worried that Obamacare will be in deep trouble—and likely be repealed—once Donald Trump is in the White House, working with Republican majorities in both the House of Representatives and the Senate. A week after the election, Trump appears to be hedging on his prior pledge to completely do away with the health reform law. What do you think will happen to the ACA—and to the millions of people who gained health insurance because of it?
The likelihood for total 100% repeal of the ACA is unlikely for two reasons: One is that this would have to be accomplished through regular legislative order in the U.S. Senate and Republicans would not be able to attract the necessary eight votes needed from Democratic senators to do this. Of course, if Republicans choose to abolish the filibuster, that would change. A second reason that repeal is unlikely is that many Republicans appreciate many non-controversial provisions in the ACA and repealing them would be backward steps they would not want to make happen.
Instead, and for now at least, Republicans appear to be moving toward a two-track process of “repeal and replace.” Repeal of the ACA’s essential health insurance coverage provisions, as well as the new taxes that financed the ACA’s expansions, could be achieved through the special “budget reconciliation process,” which only requires 51 votes for passage and cannot be filibustered. This would take some months to achieve, and is doable as long as 50 of the 52 Republican senators are willing to vote to eliminate coverage for as many as 22 million Americans—the number newly insured under the ACA—and their willingness to do that is not yet certain. Republicans did vote to repeal the most important parts of Obamacare in January of this year, but they did it knowing that President Obama would veto the measure. It would be a different vote knowing that President Trump would sign it.
Replacing the ACA with some other sort of health care law would be far more difficult because that legislation would need to proceed through regular legislative order and could and would be filibustered by Democrats, thus blocking the legislation. So it is conceivable that repeal could happen and replace might not follow, which would leave the up-to-22 million most at risk in a most difficult situation.
It’s been reported in the media that President-elect Trump may consider keeping some of the ACA’s more popular provisions, such as the requirement that insurance companies not deny coverage to people with pre-existing medical conditions, or that children up to age 26 can be covered under a family’s health plan. How do you think this might play out?
House Speaker Paul Ryan and House Republican leaders, in their “Better Way” document on repeal and replace last summer, indicated that they would continue the ACA’s “guaranteed issue” provisions—those making it illegal for insurers to deny anyone coverage because of health status, age, gender, or other factors—though only for those who are able to maintain “continuous coverage” with no or only short-term coverage breaks. For the millions of Americans who find themselves unable to afford coverage for some period of time, Republicans would, by their own words, return pre-existing condition exclusions and medical underwriting—charging the sick higher prices than the healthy. The provision for children up to age 26 being able to stay on parent’s health insurance policies is most likely not to be repealed.
How might the new president’s policies impact women’s health? He has said he would nominate a conservative Supreme Court justice who would be in favor of a pro-life agenda. Could this lead to Roe v. Wade being overturned? What other ways might women’s health be impacted under the Trump administration?
Even with a Trump appointment to the U.S. Supreme Court, there are five current votes, including Justice Anthony Kennedy, opposed to a Roe v. Wade repeal. So President Trump would need at least one additional replacement of those five to have a chance at repeal.
Other aspects of women’s health coverage are at risk because of Republican plans to repeal large portions of the ACA. Republicans want to return all discretion over required benefits to states, including the ACA’s mandates on benefits such as birth control, mammography, prescription drugs, behavioral health, and much more. So it’s possible that women could lose coverage for services that are currently free, such as contraception, mammograms, folic acid supplements during pregnancy, and screenings for gestational diabetes, sexually transmitted diseases, and cervical cancer.
Trump broke with conservative orthodoxy when he said that he’s in favor of Medicare being able to negotiate drug prices. He also has said that he would take on the Big Pharma lobby in order to reduce high prescription drug costs. Do you think he’ll be able to follow through on these pledges?
President Trump’s administration would only be able to negotiate drug prices or make other significant changes in pharmaceutical policies with the consent of Congress, which is most unlikely to provide that authority to him. Also, though the health policy section on his campaign website included drug-related proposals, the health policy section on his presidential transition website includes no mentions of these.
There were a number of health-related ballot initiatives across the nation. Three states, including Massachusetts, voted to legalize recreational marijuana and another three voted in favor of medicinal pot; voters in California, Washington, and Nevada approved various gun control measures; Californians raised cigarette taxes; and four cities voted to tax sugar-sweetened beverages. Also, Colorado rejected the establishment of a single-payer health insurance system in that state. How are these ballot initiatives changing the public health landscape?
On recreational marijuana, the tide of public opinion is changing the national landscape in spite of bipartisan opposition to this liberalization from elected officials all over the nation. It feels somewhat like the fast-changing tide a few years ago on gay marriage. And it feels unstoppable.
Taxes on sugar-sweetened beverages, at least on the local level, seem to be approaching the level of public acceptance we have seen in prior years with relation to tobacco taxes. The public seems supportive, at least in cities, especially when the revenues raised are clearly defined in terms of spending targets, such as public education. We have yet to see this approach pushed at a state initiative level, which would be a much more challenging proposition.
Regarding the vote against single-payer health insurance in Colorado, it seems that the U.S. sees one of these single-payer ballot initiatives every decade or so, and in each case, they start with some robust public support and then lose in a landslide: California in 1994, 73% to 27% no; Oregon in 2002, 77% to 23% no, and now Colorado in 2016, 80% to 20% no. It has always been a difficult sell and the Colorado results demonstrate that it still is.