If you care about transforming the delivery of medical care in the U.S., then you should should read a blog post from last week by Paul Levy, former CEO of Beth Israel Deaconess Hospital in Boston and conductor of “Not Running a Hospital.” It’s titled: “The Triple Aimers Have Missed the Mark.”
For those who don’t know, the “Triple Aim” was the 2008 invention of Dr. Donald Berwick and colleagues from the Institute of Health Care Improvement (IHI) which Berwick 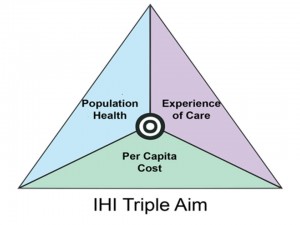 created in the last 1980s when he also developed the now-essential medical care construct of “continuous quality improvement“. As Berwick and colleagues articulated in a 2008 article in the journal Health Affairs:
created in the last 1980s when he also developed the now-essential medical care construct of “continuous quality improvement“. As Berwick and colleagues articulated in a 2008 article in the journal Health Affairs:
“Improving the U.S. health care system requires simultaneous pursuit of three aims: improving the experience of care, improving the health of populations, and reducing per capita costs of health care. Preconditions for this include the enrollment of an identified population, a commitment to universality for its members, and the existence of an organization (an “integrator”) that accepts responsibility for all three aims for that population. The integrator’s role includes at least five components: partnership with individuals and families, redesign of primary care, population health management, financial management, and macro system integration.”
One can look at the Affordable Care Act and see the Triple Aim model at work in numerous places. The key notion behind the Triple Aim is to ask: what are we trying to accomplish in the U.S. medical care system and where are we trying to go? A quick Google search will give some indication of how far and wide the concept has traveled over the past 7 years, including well beyond U.S. borders. It is a global phenomenon.
Now comes Paul Levy with a bucket of cold water: Continue reading “Is the “Triple Aim” a Part of the Problem?”